It was the best of times. It was the worst of times
Dear Friends and Family,
“It was the best of times. It was the worst of times,” Charles Dickens, The Tale of Two Cities. At Soddo Christian Hospital it is the best of times…we must be doing something right for the hospital is maxed out. But this makes it the worst of times… because the hospital is maxed out! Last month we had 92 women giving birth at our hospital, a new record. On top of the maternity rate rising, our nursing and pediatric staff are overwhelmed with the many sick babies that are born here, as well as those sick infants that are delivered at health centers and by home birth and transferred here for care. These babies born outside our hospital are admitted along with their mother into our maternity department. They require antibiotics and intensive nursing care oftentimes for up to a week or more. These patients require a hospital bed and often times a private room for heat. We do not have a neonatal nursery. Some of our mothers have to be delivered early due to severe high blood pressure or severe hemorrhage. Currently we have two babies, one born 10 weeks early and the other 11. They will require a long hospital stay to survive. By the way, most of these babies that stay here for a long time are underwritten by our maternal benevolent fund. Many of you have been so gracious to contribute to this fund. In the past our mothers went home 6 hours after delivery, but now thanks to the good care they receive from Dr. Ayers, our pediatrician and our family doctor, Dr. Becky McClaren, our healthy babies stay a minimum of 24 hours before discharge. We have 15 postpartum, GYN surgery beds in the maternity ward…compared to 30 in the other wards. This is due to the fact that we have a labor room and a delivery room and two clinics operating in the same building.
With our increase in the numbers, we are simply busting out at the seams. We stuffed another bed into our already crowded three bed labor ward. The govt. has informed us that we need a minimum of six. I couldn’t agree more, but we have no space. We have two delivery tables side by side in our delivery room. One of them is our former Gyn exam table. It is now very common to have patients recovering from their surgeries lined up in beds down the hallway because there simply are no other beds or rooms available. We have a few private rooms but they remain full. Two weeks ago patient’s families were literally fighting in the hallway to be admitted into the only available private room.
On top of the maternity increase, our Gyn patient load is escalating. During our two Gyn clinic days, Monday and Thursday, it is not unusual for me to get home at 8 PM. We then have two full surgery days on Tuesdays and Friday with a make-up day on Wednesday. All this to say….It is the best of times (because we are growing) and the worst of times, (because we are overworked and out of space)! We are working on a creative plan to add more clinic space thus creating more bed space. St.ay tuned for the details! –An update from Dr. Mark and Allison Karnes, October 2015
Two recovering surgical patients in the overcrowded hallway in the OB ward


A day in the life of a Soddo Christian Hospital team member
"A man has been stabbed in the neck. He is going to die."
These words, spoken calmly and as a matter of fact by the ICU head nurse, came as we were doing an early morning ward round prior to our planned weekend getaway to nearby Awassa. Glancing up at Dr. Ryan and Dr. Kyley, our visiting maxillofacial surgeons from the St.ates; our eyes met and without much ado, hurried to the emergency department. Reports of a large wound at the back of his neck with bone visible and a smaller wound in his anterior neck, among other injuries, made us realize that the best place to care for the patient was in the operating suite.
Meanwhile, the entourage surrounding the patient arrived in the OR with his relatives commandeering the stretcher, bringing him to the OR via the shortest route through the back door. Having gone in head first, the stretcher could not be turned around and had to be reversed into the corridor for a 180 degree spin and re-entry made, allowing a hurried transfer onto the operating table. Never mind the ABC’s of airway, breathing, etc in this race to get him to the destination.
"Oxygen, mask, laryngoscope" barks Kyley to the man standing next to him. A blank look in reply, the commands were to no avail as he was the patient's brother, not an OR worker. Amidst the chaotic, frantic activity, equipment arrived after what seemed an eternity. Blood miraculously materialized in record time, (thanks to the medical director's dash to the blood bank) and was quickly administered after a dunk in warm water. An emergency crico-thyroidotomy was necessitated to secure his airway as we were unable to effectively ventilate him with bag and mask. All along, the maxillofacial surgeons orchestrated the airway and resuscitation.
The neck injury was a through and through stab wound, entering from the posterior neck and exiting anteriorly, severing several healthy arteries supplying the posterior neck muscles. Brachial plexus, trachea, esophagus and the great vessels of the neck were spared anteriorly. Other major injuries included two deep lacerations into his left proximal thigh, a through and through laceration of one hand and another into the knuckles of his other hand.
It all ended well, the patient woke up with smiles.
[ois skin="Blog Post Share"]

Keeping Babies Warm
In Soddo, we are up above 6,000 feet elevation. So, for much of the year, it is fairly chilly. One of the challenges for us is to keep newborns warm after delivery. In the West, every delivery room has an infant warmer where the baby is placed shortly after birth. But in Ethiopia, we had struggled to find a quality product at a good price that would do this job.
That was when our pediatrician, Dr. Dave Ayer, had the great idea to make our own. He partnered with our hospital welder Yohannes, who welded a steel frame together. Then they mounted a space heater on the top of it. Voila! Our own homemade infant warmer.
[ois skin="Blog Post Share"]
Teamwork at SCH
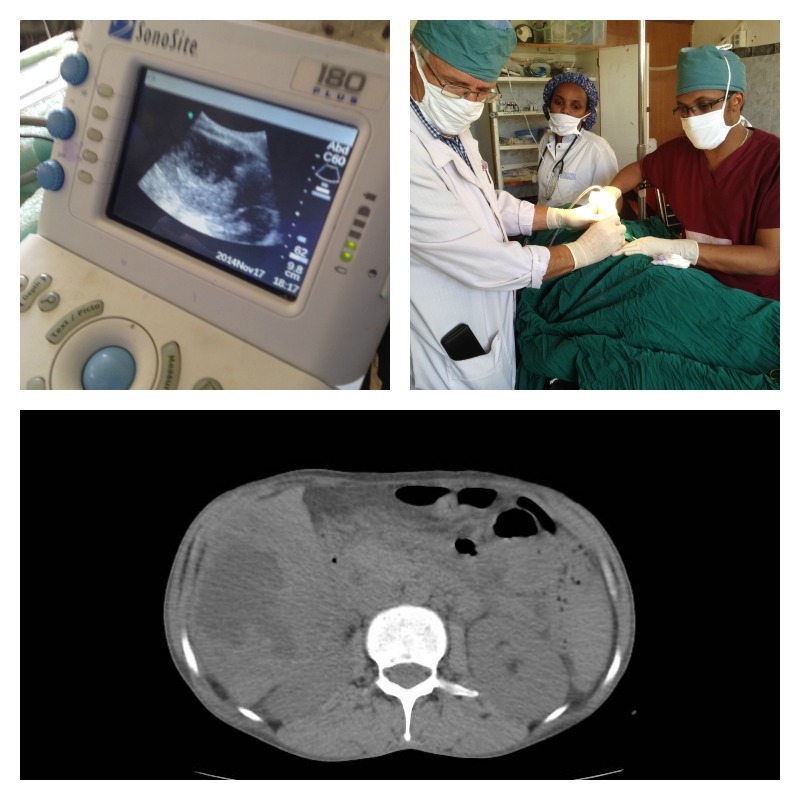
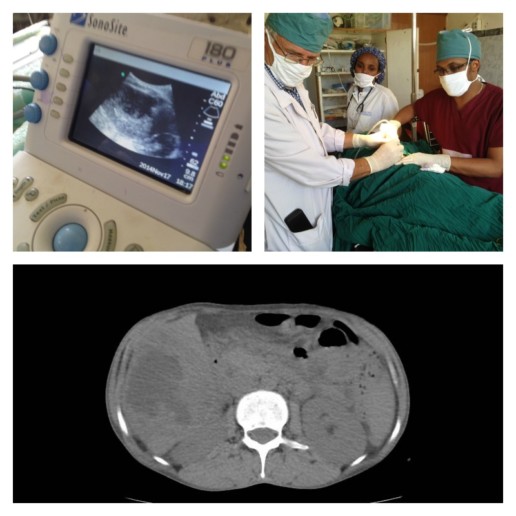
As our capabilities at Soddo Christian Hospital expand, we are working together as a team to make diagnoses, and provide cutting edge treatment for patients. The other day, we had a woman present to the Emergency Room with upper abdominal pain and fever. The ER docs did a great job with the bedside ultrasound finding what appeared to be either a fluid collection or a mass in her liver (top left picture). Then, a CT scan by the Radiology Department confirmed that it was indeed an abscess in the liver (lower pane). Finally, our expert radiologist teamed up with our surgeons (that's our chief resident Dr. Segni in the top right picture) to do an ultrasound-guided percutaneous drain. This is a minimally invasive way to get the infection out instead of a big operation.
We are so proud of all of our services working together to get the best outcomes for patients! Praise God for new technologies and teamwork!
[ois skin="Blog Post Share"]

Medicine + the Gospel - History of SCH Pt. 4
In 1946, the missionaries returned to Soddo, having found a vibrant church had grown in their absence. In addition to this, they reoccupied the hospital they had started before - having to kick out some livestock who had taken up there!
In the following decades, the ministry of the hospital grew. What had begun as primarily a church planting ministry, now evolved into a medical ministry - ministering to the sick and dying in an effort to preach to them the Gospel of Jesus. Dr. Barlow and other physicians cared for burn and trauma patients, obstetric emergencies, malaria, typhoid, leishmaniasis, schistosomiasis, and a whole host of other conditions. The hospital grew to 105 beds to care for the sick of Wolaitta and the surrounding areas. The Gospel was shared, and many came to know Christ.
The conditions were meager, such that in 1967 when Dr. Harold Adolph joined the staff, he described a hospital with walls made from mud and sticks covered with "bamboo mats to keep them from oozing when it rained." The operating room light was a single light bulb dangling from a rusty coat hanger. The OR table only had three legs, with a some scrap pieces of lumber cobbled together for the fourth. In fact, the one sterilizer they had exploded, forcing the surgeons to use the largest pressure cooker they could find to sterilize instruments.

The need for a new hospital was great. And SIM and the doctors began raising funds for that purpose in the late 1960s. By 1975, the new hospital was complete having been built in a period of seven years by five different contractors. Dr. Adolph and the others, however, would barely have any time to enjoy their new facility. In 1974, a coup d'etat forced Emperor Haile Selasse from the throne and brought to power a harsh military and then Communist regime known as "the Derg". Aligning itself with the Soviet bloc, the Derg became hostile to any Western influences, and forced the missionaries to leave the country in 1976. They then took over the new hospital which SIM had built and made it a government hospital. Only God knew then if a medical ministry would return to Soddo someday. St.ay tuned...

This is the fourth installment in a series of posts about the history of SCH.

A Church Born in a War - History Part 3
When we last left our story, the missionaries in Soddo were seeing new converts under the looming threat of war. What had once been a stronghold of Satan worship and paganism, was beginning to see its first evangelical church!
In February of 1935, the missionaries began building the first mission hospital in Soddo. Only eight months later, the Italian General de Bono marched into Ethiopia with troops without even a declaration of war. The occupation was underway, but in remote Wolaitta Soddo, the missionary work continued on. News came to the missionaries in Soddo as various events unfolded. They worked ever harder to win more and more converts to Christ, knowing that their time in the country may be limited.
On May 5, 1937, Addis Ababa fell to the Italian invaders. It was not known how long, or even if, the invaders would make their way to the southern regions. But they did, and on January 19, 1937, Soddo itself was occupied with Italian troops. Just three months later, the missionaries were forced to leave. Nineteen adults and seven children boarded an Italian army convoy which took them to Addis to depart the country.
In those two years between the first rumblings of war and the evacuation, God added several dozen new converts to the young Soddo church. It was not known what would happen in the years that followed. What ensued was a vigorous persecution of the new Christians. Wandaro himself was jailed and beaten almost to the point of death. As other leaders were imprisoned, and yet stayed strong in their faith, it only gave credibility to the young church. The gospel spread like a wildfire, and converts were added by the hundreds, and then thousands.
In 1945, as World War II ended and the Italians had been defeated, missionaries started to return to Ethiopia. Upon arriving to Soddo, they were greeted and welcomed back by the thousands of Christian believers in Wolaitta. Over 150 churches had sprung up in their absence. They rejoiced to see what God had done in the midst of the suffering that had taken place. A huge vibrant church had been born!
The new converts had done the best they could with no missionaries around. Some rather humorous practices had developed. Some of them recalled seeing only believers at Communion. So the first Wolaittan church adopted the custom of dismissing all non-Christians when the Lord's Supper was served. And they swore the participants to secrecy - not to describe the Lord's supper to anyone. They had also stopped raising goats - due to Jesus's warning that the "goats" would be sent to eternal damnation in Matthew 25!
They had to wait until the fall of 1946 before they were permitted to move back onto the old mission station. At that point, all of the hospital and the residences had been occupied by squatters and their animals. The Ohmans, now with Dr. and Mrs. Nathan Barlow, began taking possession of the hospital back, and gradually restored the place to a usable condition. Even though it would be a while before they could start doing surgery again, the word of their return traveled fast, and already patients were lining up to be seen.
[ois skin="Blog Post Share"]
History of the Mission to Soddo, Pt. 2
How is a church born? In Soddo, it happened like this:
In 1928, the Lambies had arrived in Soddo to set up the mission station. Along with them were the Rhoad family, and three single men: Glen Cain, Walter Ohman, and Clarence Duff. They were invited to set up their homes in a place called Otona which sat atop a foothill just to the east of Mt. Damota. (Soddo sits in the shadow of Mt. Damota which was named for a previous king in this area).
They set to work building their homes which were made of local materials. According to SIM's policy, they were to have the luxury of a bathtub and a cook stove in the home, "so as to add to the missionaries' comfort." They spent their days in the homes of the Wolaitta people, learning their language with one goal in mind: to be able to formulate a Gospel presentation to the people. They established a clinic to provide practical help to the people in that area as well.
In 1929, their forces expanded. The mission team was joined by the Lewis family, Selma Bergstren, and a nurse named Ruth Bray. Within two years, the team had learned the local language enough to present the Gospel. They began preaching at Otona to those who were coming to the clinic - combining physical and spiritual ministry just as we do today at Soddo Christian Hospital. One day, a young man named Wandaro happened to come by and hear the preaching.
Wandaro was from Humbo, a little south of Soddo, and his father was a well-known witch doctor there. On that day, Wandaro had been on his way to the market at Soddo, when a terrible thunderstorm hit, and he ducked into the clinic in Otona to get out of the rain. It was there that he first heard the Gospel, which he said sounded like "honey to his stomach." He was drawn to the message, and a week later went back to hear more. After a third visit, he professed faith in Jesus Christ, and the first Wolaitta believer was born.
In the years that followed, many more professed faith in Jesus, and the missionaries were baptizing new converts regularly. The Lewises lost a baby son three days after birth, and many Wolaittans came to mourn with them. In the wake of this tragedy, many locals became Christians after observing the peace that the mission team exhibited in the face of such tragedy.
By 1936, there were 73 believers in Soddo. The mission had expanded to neighboring villages as well like Koisha, Yirga Alem, and Arba Minch. It was estimated that in all of this southern region, they had seen close to 150 conversions. But the tide of war was sweeping into Ethiopia. The Italians had invaded, and the missionaries were going to be forced to leave. Many of them left with a sadness. Despite what they had seen, they feared it wasn't enough to birth a new church yet.
But God had plans for the Soddo church...
[ois skin="Blog Post Share"]
History of the Mission to Soddo, Pt. 1

At SCH, we are standing on the shoulders of Christian pioneer missionaries and missionary doctors who went before us. As we approach our ten-year anniversary in a few months, we thought we’d take a look at where we began, and how far God has brought us.
Dr. Thomas Lambie was a medical missionary with the American Presbyterian Mission working among the Sudanese Nuer people. In 1918, he became the first American missionary in Ethiopia when he sailed up the Baro River and began working among the people of the Wellega region. He labored there for the next 10 years, founding a hospital, a school, and a vibrant church. At this point, he combined forces with two other missionaries – Albert Rhoad and George Buxton - and founded Abyssinian Frontiers Mission.
Now at that time, Christianity had not made its way into the southern part of Ethiopia. At least fifty different people groups occupied the south, and most were engaged in animistic worship and witchcraft. Some accounts say they were devoted to the occult and the “worship of Satan”. Dr. Lambie and his colleagues were deeply burdened by this and desired to penetrate this area with the Gospel. Abyssinian Frontiers Mission merged with the Sudan Interior Mission (SIM), and was given permission to set up a mission station in the South. The most logical place at that time was Soddo.
The governor of Soddo was a man named Dejazmatch Yigezu who providentially had been a patient of Dr. Lambie’s in Wellega. He remembered the doctor, and welcomed the missionaries. (In addition, the missionaries had the support of Emperor Haile Selassie since the magistrates of Wellega had spoken highly of them). The mission station in Soddo was established by 1929, and evangelistic efforts were spreading out from there to Sidamo (Yirga Alem), and Gamo Gofa (Arba Minch).
It should be noted that Soddo was chosen as the main hub because of its easy access to Addis Ababa. At that time, it took two weeks with a mule caravan to reach Soddo from Addis. But this was considered a good distance for fetching supplies, and yet still to be a good launching point to reach the South!
In the next post, we'll tell you how the Church in Soddo began under the mission work of the Lambies and others...
[ois skin="Blog Post Share"]
Neurosurgery at SCH?!?
What do you think happens when you combine the following:
- A country with the highest number of pedestrians struck by vehicles relative to cars on the road
- A brand new CT scanner among a population of 5 million people who previously had none
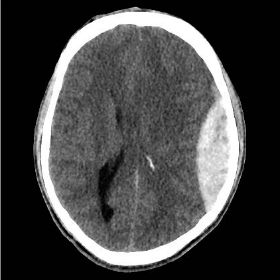
If you answered, “a lot of new diagnoses of head trauma”, you’d be right. Our CT scanner is practically smoking with all the head CTs for trauma that are being done. Most of the time, we find non-operative bleeds. But the last two weeks has been extraordinary. In September alone, we have taken seven patients to the OR with epidural and subdural hematomas that required emergency surgery.
 Above are just four of the actual scans done here in the past two weeks. And there are more! We’ve had great outcomes so far, and our surgery residents and staff are doing more emergent neurosurgery than they ever could have imagined.
Above are just four of the actual scans done here in the past two weeks. And there are more! We’ve had great outcomes so far, and our surgery residents and staff are doing more emergent neurosurgery than they ever could have imagined.
We praise God that He provided through our donors. Through your generosity, we got a CT scanner. And it is being used for His glory as lives are being saved. May the name of Christ go forth in southern Ethiopia as we use this gift. That is our prayer.

Empowering the Next Generation
Imagine a missionary doctor sitting under a tree in Africa, seeing patients as they line up from far and near. She sees 100 patients a day or more. In a year, perhaps 3000. In ten years, 30,000. Not a bad contribution to the problem of suffering in her country. But imagine how burned-out, how completely exhausted she is after this work. And when she finally gives up, the work is finished. Many thousands of patients were treated, and many lives saved even. But the work is not enduring. It is not sustainable.
Now, imagine that same doctor pouring her life into doctors-in-training in that country. Year after year, spending intentional time teaching 10-15 resident physicians. In ten years’ time, perhaps 20 or 30 are trained. Each of those go on to treat thousands of patients in their careers. Some of them are retained as teaching physicians, and they in turn pour into others. This is multiplication. This is empowerment. The impact of that one person is perhaps 50-fold when compared to the lone worker at the beginning of our story.
This is what we do at Soddo Christian Hospital through PAACS.
The Pan-African Academy of Christian Surgeons was founded in 1996 with one residency program in the jungles of Gabon. Since then, it has grown to twelve programs in ten countries. We are one of those programs. Why is it so important to train African surgeons?
Right now, 56 million people in sub-Sahara Africa are in need of surgery. In most of the continent, there is one surgeon for every 250,000 population. In Ethiopia, there are only a 300 surgeons for a country with almost 90 million inhabitants. (If WHO guidelines were met, we would have 4,150!) PAACS has the goal to train 100 surgeons by 2020. Thirty-six have been trained thus far, and God-willing, the goal will be met by 2019.
Because the program is fully accredited, our graduates are eligible to be members of the College of Surgeons of East, Central, and Southern Africa. And in turn, are fully licensed by the country of Ethiopia as surgeons. And the faculty actively disciple the residents during their training - teaching them not just excellent surgical practice, but equipping them with the spiritual tools to use medicine to bring people to Christ.
We praise God for this kind of empowerment and training. Of Africans. For Africa.