Sustainability, Mission Hospitals, & the Early Church
How do you do medical missions in a sustainable way? Medical care is expensive, and providing it to the poorest of the poor is financially implausible. And yet, those with a Christian worldview know that God commands us to "act justly and to love mercy" (Micah 6:8). Basic economics teaches us that doing so will come at a cost. And who is to bear that cost? Well, we learn in Acts 4:32-35 that the early Church had a good solution for this. They were sharing their possessions with each other "as they had need." This may be the reason (according to Rodney Stark and others) that the early church grew in such an explosive fashion. As new Christians met the needs of others in the Body, the world was watching. This kind of selfless compassion was contagious, and new followers were added to their numbers daily.
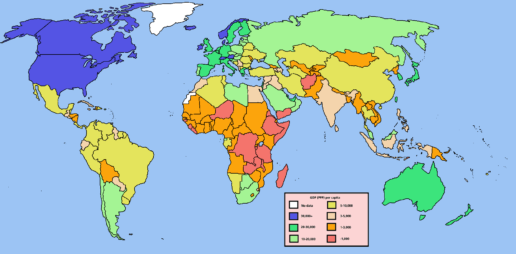
The map shows the per capita GDP (gross domestic product - a measure of economic output) across the globe. North America and a handful of Western European countries represent the wealthiest. Ethiopia and other Sub-Saharan African countries the poorest. We find members of the body of Christ in all of these places without respect to political boundaries. If you live in a "blue" or a "green" country, do you feel a new weight of responsibility? So, as Francis Schaeffer famously asked, "How should we then live?"
Soddo Christian Hospital does not provide care for free. Some mission hospitals do, but ours charges a small fee. We believe this to be important to the longstanding sustainability of the hospital. (That's another post for another day.) But that alone is not sufficient to run a hospital. We have pledged as an institution to offer "excellent medical services," and that we intend to do. But the economy in which we work is not able by itself to support this lofty vision.
And so we turn to you. We need your help. We need the Body of Christ in the "blue and green countries" to step up and say, "We'll take care of it." Someday, we hope that the economy in rural Ethiopia will be booming, and will fund the hospital fully. But until then, we know others will have to stand in the gap. Is that sustainable? Well, perhaps it is, and perhaps it isn't. If you have thoughts on the subject, we invite you to comment below.

Does a mission hospital treat everyone?
This is a question that we get asked a lot. So we wanted to address it. And the answer is... yes!
Our hospital is a mission hospital. You can read all about our mission and values here. But suffice it to say, that we exist not just to treat people with excellent medical care, but to proclaim the Gospel of Jesus Christ and make disciples.
But do we treat anyone who comes in the door, no matter what their faith or background? Of course we do! We are proud to serve the people of this part of Ethiopia. Fortunately, as our reputation has grown, now we are also seeing patients referred to us from all over the country. And these patients come from all types of backgrounds. Some are Ethiopian Orthodox, some are Muslim, some are animistic, and some are Protestant. We see and treat them all.
In the hospital, our staff will offer to pray with patients regardless of their background. We believe that a person's health should be attended to physically and spiritually. We find that our patients really respond to the fact that we care about them in this wholistic manner.
Often, if a patient is open to hearing about it, we will share with them the life-giving message of the Gospel. We don't force it. But we do give them the opportunity to hear. We play the Jesus Film in the hospital. We will often provide a Bible in Amharic. By God's grace, we have seen over 500 patients profess faith in Christ since the hospital opened its doors. But even for those that kindly decline, we aim to provide excellent care just the same.