
Putting Our New Gifts to Work!
Recently, we started running our brand new CT scanner. And it's already making a huge impact in the way we care for patients. We were also able to purchase an ambulance recently, and that too is making a difference. Let us tell you about one such patient whose life was just saved because of these gifts to our hospital.
Yohannes was a victim of a car accident. A terrible car accident that had fractured several of his ribs, and resulted in a punctured lung. Even with supplemental oxygen and a chest tube, we were not able to keep up the oxygen level in his blood. From the x-ray we suspected that he might have lung contusions - a severe bruise to the lung itself - that makes it impossible to breathe. But it wasn't completely clear. Maybe something else was going on? Our surgeons considered taking him to the operating room to open up his chest - a procedure called thoracotomy. But because of our CT, we were able to scan his chest, and the result saved him a brutal surgery. The CT in fact showed severe lung contusions - something that would not be helped with surgery.
So, now what to do with Yohannes? We don't yet have a mechanical ventilator (although we will soon thanks to more donations). So, the only hope for him was to get him to Addis Ababa and a hospital with mechanical ventilation. It was nearing dusk, and the helicopter from nearby Awassa was not able to airlift him there. And so, our brand new ambulance made its maiden voyage to Addis with a patient.
We intubated the young man, and his oxygen levels improved immediately with the bagged air forced into his lungs. One of our anesthetists rode in the back, squeezing the bag for six hours all the way to Addis! He got to the hospital there in the middle of the night, and got placed on a ventilator. I spoke with the ICU doctor at the accepting hospital today, and though he is critical, he has a fighting chance for survival now. If he can be mechanically ventilated while his lungs recover, he just might make it!
This kind of care is only possibly because of our generous donors. Our hearts are filled with gratitude for those of you who made it possible for us to get a CT scanner (which saved this young man a surgery) and an ambulance (which got him to an ICU that could care for him).
Be a part of the team. Join our 100 for 100 campaign today! Pledge $100 monthly gift for the next year, and be a part of the 100 donors who are saving lives in Ethiopia.

On Her Own Two Feet
Imagine being 27 years old and having never walked upright. That was the plight of Mihret. She had been born with a congenital knee dislocation in both legs that made it impossible for her to stand on her own two legs. I saw her in the ER one day recently. She came from Addis Ababa - the capital city five hours away. And she had heard that our hospital was working miracles for people who had never walked. Her entire life, Mihret had crawled on her hands and knees. She wore flip-flops on her hands to protect them from the hot city pavement.

She was poor, and didn't even have enough money to get x-rays taken of both knees. We worked out a deal so she could at least get the x-rays and talk to our orthopedic surgeon about treatment options. Since birth, her dislocated knees had only flexed in the wrong direction, making it impossible to stand. But Dr. Anderson saw her in the clinic and felt like if her knees could be fused, she could stand, and even walk with assistance.
She didn't have a penny to pay for such a surgery, but our Benevolent Fund covered her.
A week after admission, she underwent the first surgery on the left leg. A complex procedure that lasted hours and involved putting a rod through her femur, bridging the distorted knee, and going into the tibia. Mihret lost a lot of blood, an issue complicated by the fact that her blood type was O negative - the most rare type. But she got transfused, and recovered for three weeks before having the right side done. According to Dr. Anderson, "With the experience on the left side, we were able to do the right side without as much bleeding."
Just a few days after that, for the first time in her life, Mihret stood upright on her own two legs.
We have a weekly chapel service at the hospital on Wednesday morning that is attended by most of our hospital staff. We gave Mihret the opportunity to attend chapel, but not just attend. To walk down the center aisle. Never before has our staff reacted to a patient's recovery like they did with her. There was exuberant cheering and applause, and some of our staff cried as Mihret gave thanks to them and to God. A day of rejoicing at Soddo Christian Hospital that will not soon be forgotten.
All of this was possible because of our Benevolent Fund. And you can be a part! We are actively recruiting donors to give on a recurring basis. Right now, we are looking for 100 donors to pledge $100 per month for the next year, so that more like Mihret can get life-transforming treatment. We are giving ourselves 100 days to find these donors. Join the team today!
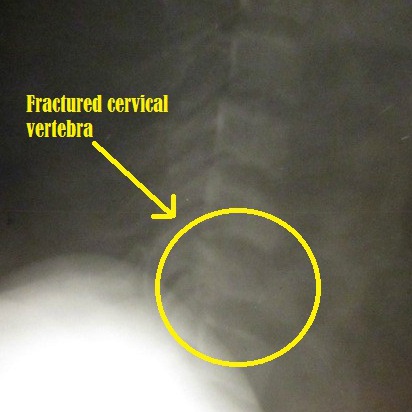
To Walk Again
This is what a broken neck looks like:
About seven months ago, a 17-year old young man came to us after an injury. What you see above is his actual x-ray. He had been in a tree, and fallen quite a distance. He had a fractured femur, but worse than that he had a broken neck that had caused paralysis. He could not move his arms or legs, and only had some preserved sensation in his extremities. We surgically repaired his leg and his neck, and he was in the hospital for one month recovering. Sadly though, even at the time of his discharge, he was barely moving his fingers and toes. We were unsure if he would ever walk again.
Recently, the young man returned for his follow-up. Praise the Lord that he is now almost fully recovered. He has almost full strength in his arms and hands, and can run on his own two legs. A paralytic healed! Here he is pictured below with Dr. Anderson.
The best part of the story is this. This young man was quite poor. He was unable to pay for his care. But because of generous donors to the Benevolent Fund, his surgeries and post-operative care were paid in full. Because people like you care enough to give, we were able to medically care for him. By God's grace, he is healed and planning to return to school later this year.
Help us treat more patients like this! Our Benevolent Fund relies on donors like you. And 100% of every dollar goes to fund patient care. We are looking for 100 donors to pledge $100 per month for the next year. These funds will help us to cover the costs of our poorest patients. You can set up a recurring gift through our secure site here. God bless you!

The Work of God
Two of our staff go out into the rural areas around Soddo every week to deliver much needed prenatal care. Over 95% of women in rural Ethiopia will deliver their baby with no professional attendant - midwife, nurse, or doctor. Even more than that will have no prenatal care at all. These are the reasons that we continue to see high maternal mortality and neonatal mortality in this country. (A woman aged 15 has a one in 67 chance of dying in childbirth. In the US, it is one in 2,400.)
Well our staff are doing something about it! Every week, Sophie and Jodi head out "into the bush" to tend to these pregnant ladies. Women come from all over, and line up to see them. Occasionally, they will see a critically ill mom who needs prompt attention - those get referred on to the hospital. One such woman came last Thursday.
Her complaint was that "water was coming out," and indeed she had what we call "premature rupture of membranes" - her water broke too early. She was only seven months pregnant. Not only that, but she had lost two babies before. Both at exactly the same time - seven months.
They loaded her up in the car, and brought her straight to Soddo Christian Hospital. She was seen by Dr. Mark Karnes, our obstetrician, but the situation looked grim. She was admitted, but a few days later went from bad to worse. She abrupted her placenta (where the placenta tears away from the uterus), and began hemorrhaging. It required an emergency C-section. (Dangerous for mom because of the bleeding. Dangerous for baby because these little ones often don't have developed enough lungs to survive once they are out of the womb. They lack something called surfactant which keeps the air sacs open in the lungs. Fortunately, if the mom receives steroids in the hospital, this problem can be helped.)
A beautiful little girl was born, weighing less than three pounds, but breathing on her own - only occasionally requiring oxygen support. Her mom couldn't be more thrilled, and is cuddling her close to her body to keep her warm. Something that is called "Kangaroo Care." And the new little one's name says it all - Yabsera. Literally "the work of God".

SCH Graduate Makes History
Recently, the very first graduate from the PAACS program in Ethiopia did something unique in his own country. He led a team that separated conjoined (“Siamese”) twins. To our knowledge, nothing like that had ever been attempted in Ethiopia. Dr. Frehun Ayele, who trained as a pediatric surgeon at the BethanyKids at Kijabe Hospital PAACS program after graduating from the general surgery program in Ethiopia, led a team of surgeons from Myungsung Christian Medical Center to perform the incredibly delicate and complicated operation. The baby sisters were born at a health center in the countryside and were abandoned by their mother. They were given to a Catholic mission group here who then brought them to MCM. One of the twins had a severe, fatal heart defect and it soon became clear that she could not survive. This made transfer abroad impossible because of time considerations, so Frehun made the difficult decision to take them to the operating room to separate them. It was clear that one of the twins would die, sacrificing her life for her sister's. Dr. Frehun concluded that if he did not intervene urgently, both babies would die. The surviving twin, Mariam, is doing well. Please pray for her as she recovers. We praise God for Frehun's faithfulness in serving Him as he serves the sick children of Ethiopia.


Hot Zone in Soddo
Last week, we had some pediatric patients come in with upper respiratory symptoms. A few of them had a rash and had been given antibiotics, so there was a thought that maybe it was a "drug-related rash." But it wasn't long before a few more kids came in, and it was clear that this wasn't a medication-induced rash. Yep, this was measles.


It didn't take long before our entire pediatric ward was full of measles patients. We were in the middle of a genuine outbreak. The feared complication of measles is pneumonia, and indeed most of the patients we were getting had it. Many have them were requiring oxygen. In the picture below, the machines on the floor are oxygen concentrators.

The health department was notified, and they began taking measures. Much of the outbreak was centered on an orphanage down the street from us. So we contacted them and gave them specific instructions. First, isolate any kids that were showing symptoms. Second, send any kids to the hospital that were showing signs of pneumonia or respiratory distress. We took a trip down to the orphanage ourselves to see the patients who were not sent to the hospital and check on them.

By God's grace, the outbreak seems to be relenting. Our hospital has admitted around 15 kids. Sadly, a few of them have succumbed to the disease. The thing about measles in outbreak settings, is that it affects the very young. Children are vaccinated against this virus between nine months and one year of age. So the most vulnerable are the babies less than nine months. Formula-fed babies (like the orphans) are particularly vulnerable because they don't get protective maternal antibodies. Fortunately, some who were very sick are pulling through. The situation itself feels like a war zone. Our doctors and our nurses are tired, but they are doing an amazing job - rising to the occasion and providing excellent care. We praise God for using us in this situation, and hope to bring Him glory through it. As it says in 1 Cor 15:58, "Be steadfast, immovable, always abounding in the work of the Lord, knowing that in the Lord your labor is not in vain." Pray that we will be steadfast. And that no more of these precious little ones will die.
The other thing about situations like this, is that it stretches our thin resources to the maximum. We don't have enough oxygen concentrators. We don't have enough pulse oximeters. And we can't mechanically ventilate kids with severe pneumonia. We hope to buy non-invasive ventilator machines, and perhaps one or two mechanical ventilators. We'd love to be even better prepared the next time this happens. Would you consider a donation today that would help us do that? Just click donate in the upper right corner of the site. Thanks for your support and prayers.

One in a Million Babies
One in 729,000. That is the odds of having quadruplets naturally - without the aid of fertility medicines. And for this young Ethiopian lady, it happened 5 days ago. With no prenatal care, and no knowledge of the multiple babies she was carrying, she made the trek from her rural home to the local health center. There she gave birth to four babies, one of whom died soon after birth.
She was advised to seek further care at a hospital, and found her way to us. The mother herself is being treated with antibiotics for a suspected uterine infection, but she is expected to make a full recovery. The three surviving kids are doing well. Two of them have a mild omphalitis (an infection of the umbilical cord stump) and are being treated with IV antibiotics. They are expected to do well.
The three celebrated the Ethiopian New Year yesterday on their fourth day of life. The new family is the talk of the hospital as we ring in the New Year. A multiple gestation pregnancy is high-risk in any country, but especially here where over 90% of the women have no access to prenatal care. Though we mourn the loss of one of the babies, we praise God for the miracle of a healthy mom and three healthy infants.

A Miracle at Soddo

The parents were shrieking in grief and disbelief as they ran their 14 month old little boy to the ER at Soddo Christian Hospital.
Just minutes earlier they had found him upside down in a bucket. A bucket of mop water. He had wandered out and managed to tip himself into it, and couldn't get out. He literally drowned.
When the parents brought in little Yekebesera, they thought he had been underwater for at least five minutes. In the ER, he was having seizures which were requiring multiple doses of strong medications to stop them. Only minutes later, he began "posturing" - meaning that he was extending his arms and legs in such a way that indicates very severe brain damage.
Our pediatrician admitted him to the ICU, and assisted his breathing with a CPAP machine which we just purchased through generous donors. All of the doctors who cared for him that evening thought this little boy would never make it. But trusting God, and hoping for a miracle, we did everything we were capable of doing.
The next days, Yeke remained seizure-free, and started waking up more. Here's what our pediatrician Dave Ayer said when he walked into the room on hospital day #3:
"When I came in Sunday morning and his dad asked me if he could eat...I thought he was joking. That is, until I looked down and found out this little guy had purposefully ripped off some of his monitoring equipment. He was interacting normally with his parents and requesting something to drink. It nearly brought me to tears--today he came off CPAP and is on minimal oxygen support and eating/drinking like a normal kiddo. My only remaining challenge will be to convince his dad that he actually needs to stay 7 days to finish his antibiotics."
Praise God for this miracle. And for donors like you who gave so that this boy could have the gift of life.