
21 New Hips!
Recently, we had the privilege to be visited by a joint specialist from the US. Dr. Clint Barnett is an orthopedic surgeon at the Scott & White Medical Center in Temple, Texas. He specializes in replacing worn out knees and hips in patients who have suffered from severe arthritis and debilitating pain.
Last week, he brought those skills to Ethiopia and Soddo Christian Hospital. In just one week, he and Dr. Anderson and our OR crew knocked out 21 hip replacements! Yes, that's right. Twenty-one!
21 patients who had been suffering for years with severe pain.
21 patients who could barely walk.
21 patients whose lives will never be the same.
We are so proud of our OR team as well. These anesthetists, scrub nurses, porters, autoclave staff, and recovery room staff worked extra hours and on weekends to get the work done! Near the end of the campaign, we had a couple of the patients come up to the front of our weekly chapel service to share how they were already feeling better.
At Soddo Christian Hospital, our desire is to provide excellent medical services and make disciples of Jesus Christ. We are thankful that God sends servants like Dr. Barnett our way, and pray that God will all the glory for the work that is done here in Soddo!

One Day Too Late
"If only she had come in one day sooner." I can't tell you how many times I think that here. Elfinesh was a 32 year old woman in the prime of her life, with a loving husband and two small children. She came in to the emergency room with a history of four days of vomiting. The illness, abrupt in onset, had taken a horrific toll on her body in such a short time. It was probably sepsis - when an infection spreads rapidly through the body via the blood.
We worked as hard as we could. Three of our staff doctors and two of our nurses attended to her simultaneously. Placing IV lines, giving fluids, antibiotics, running tests. Elfinesh clung to life, but she was so far gone that she was in a coma and unresponsive to anything. A few hours into her course, she stopped breathing. We tried to support her breathing, and when her heart stopped, we tried CPR. Unfortunately, our attempts came to nothing, and after about four hours, she passed from this life into the next.
I wish I could tell you this was a rare occurrence. But the reality is that in a country where access to medical care is sorely lacking, many patients wait too long. Maybe they live several days' walk from the nearest health center. Maybe they have no money to scrape together even the $2 that it would take to see a doctor. Perhaps they are delayed by traditional and cultural healing practices that actually exacerbate the problem. The barriers to care are numerous, and as a result, many suffer. All of our providers can tell stories of patients who came in just a day too late.
You see, there are no Minute Clinics in Ethiopia. In our region of 3 million people, there are only two hospitals. There are no accredited laboratories. In a country of 90 million people, there are only 18 CT scanners. There are NO cardiac surgeons. Consider even the lack of the most basic of health care needs - trained general practitioners. In Ethiopia, there is only one doctor for every 50,000 population. (In the US, there are 100 times as many providers per capita).
We are working to address these issues. Not only are we providing care, but we are training in order to build capacity. But we need your help! With funding, we can provide more training and more service. We can expand access so that there are fewer stories that end like Elfinesh's. Help us help Ethiopia.
Happy World TB Day 2014!
You probably haven’t heard much about tuberculosis, or TB. Maybe you remember that Nicole Kidman’s character Satine in Moulin Rouge died from TB. Or you remember Katerina Ivanova in Dostoevsky’s Crime and Punishment. But you probably don’t personally know anyone with the disease.
But the fact is, TB is everywhere. Epidemiologists estimate that 2.3 billion people in the world are infected with TB. Let that sink in for a minute. Two point three billion. Fully one-third of the world’s 7 billion population.
Why have you not heard much about it then? Well, because in the US, less than 1% of the population has been infected with TB.
The thing is, TB is a disease of the developing world. Every year, 9 million new people are diagnosed with TB disease – and 98% of them live in the developing world. Nelson Mandela said, “The world has made defeating AIDS a top priority. This is a blessing. But TB remains ignored. …We can’t fight AIDS unless we do much more to fight TB as well.”
In the emergency room in Ethiopia, I see TB every single day. Literally. Last week, I saw a woman come in with abdominal pain who had lost a fourth of her body weight. She looked like a skeleton. Her abdomen was rigid and tender, and it turned out she had TB infection of the intestines. Another day, I saw an adolescent with back pain because TB had destroyed his spine (we call this Pott’s disease).
This is the kind of stuff that you only read about in textbooks in America. But in Africa, it is deadly real. Ethiopia is one of the “high burden” countries for TB – 22 countries which make up 82% of the entire world’s cases . In Ethiopia, there are 280,000 new cases of TB diagnosed every year. Epidemiologists call this “incidence”. (By contrast, in the US, there are about 10,000 new cases of TB every year). The Millennium Development Goals are seeking to reduce TB in countries like Ethiopia. But the political will is lacking. There are few high profile celebrities with TB. Research dollars that go toward TB are dwarfed by that of HIV. Though we have countless new drugs for HIV, we have NO NEW DRUGS to treat TB.
What can we do to fight TB? For centuries, the only way to diagnose it has been by looking at someone’s sputum under a microscope. And this only catches TB 50% of the time! (In contrast, the test for HIV is in the blood, and is 99% accurate at detecting the disease). Finally, in recent years, a device has been developed that can confirm TB. It is called the GeneXpert, and we hope to get one here at Soddo Christian Hospital.
So today, on World TB Day, perhaps you find yourself asking, “What can I do to help stop TB?” Well, if you’re a friend of Soddo Christian Hospital, the answer is surprisingly simple. We would like to get a GeneXpert. It will make diagnosis of the disease more accurate, and allow us to help many more people. We will detect when patients are suffering from this horrible disease, and can start lifesaving therapies immediately.

Barnabas' St.ory
 Every Wednesday morning, the hospital staff at Soddo Christian Hospital gathers together before work for a chapel service led by the chaplains. Songs are sung, the Word is opened, and testimonies are shared. For our team, here only a short time, it was a highlight in a week full of highlights, because we heard the joyful testimony of a teenage Ethiopian boy whose mother is receiving care at the hospital.
Every Wednesday morning, the hospital staff at Soddo Christian Hospital gathers together before work for a chapel service led by the chaplains. Songs are sung, the Word is opened, and testimonies are shared. For our team, here only a short time, it was a highlight in a week full of highlights, because we heard the joyful testimony of a teenage Ethiopian boy whose mother is receiving care at the hospital.
This young boy, whom I’ll call Barnabas, is from a rural area of Ethiopia that lacks infrastructure and educational opportunities for children. In fact, he said, in his home region education is not prized and many are hindered from pursuing one. In his longing to receive an education, he attended a school started by Christian missionaries, where he heard the gospel and became a follower of Jesus.
However, when Barnabas told his family about his decision, they forced him to choose between his family and his faith. He chose faith in Christ, experienced persecution and isolation, and was forced to leave his home. Barnabas moved around, staying with people he hardly knew, all the while growing in his knowledge and love of Jesus.
Barnabas soon received the news that his mother was sick. He returned home and tried to find her health care locally and then at a referred hospital in Addis, but no one could help his mother. Finally a doctor referred him to Soddo Christian Hospital, saying simply, “They can help your mother.”
Barnabas spent the last of his money getting his mother to Soddo. He handed his mother’s care to the doctors and nurses at Soddo Christian Hospital, so grateful that she could be served with the love of Jesus Christ. While his mother is treated, Barnabas has spent his time at the hospital sharing the gospel with patients and their family members, believing strongly, as he says, that “Jesus is the only way. He is the Way, the Truth, and the Life. He has given me life.”
Through the love shown to her at the hospital, Barnabas’ mother, who once forced her son to leave because of his faith, has decided to become a follower of Christ. In Barnabas’ words, he “once was just one” in his town and family, but “now we are two.”
With that, the listening chapel congregation burst into applause, rejoicing that God sees and saves all that desire Him, but also knowing that Barnabas and his mother are not just two but join the multitude of brothers and sisters all across the world who call Jesus their Lord.
To Walk Again
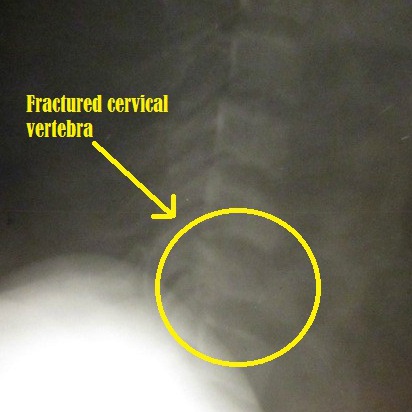
This is what a broken neck looks like:
About seven months ago, a 17-year old young man came to us after an injury. What you see above is his actual x-ray. He had been in a tree, and fallen quite a distance. He had a fractured femur, but worse than that he had a broken neck that had caused paralysis. He could not move his arms or legs, and only had some preserved sensation in his extremities. We surgically repaired his leg and his neck, and he was in the hospital for one month recovering. Sadly though, even at the time of his discharge, he was barely moving his fingers and toes. We were unsure if he would ever walk again.
Recently, the young man returned for his follow-up. Praise the Lord that he is now almost fully recovered. He has almost full strength in his arms and hands, and can run on his own two legs. A paralytic healed! Here he is pictured below with Dr. Anderson.
The best part of the story is this. This young man was quite poor. He was unable to pay for his care. But because of generous donors to the Benevolent Fund, his surgeries and post-operative care were paid in full. Because people like you care enough to give, we were able to medically care for him. By God's grace, he is healed and planning to return to school later this year.
Help us treat more patients like this! Our Benevolent Fund relies on donors like you. And 100% of every dollar goes to fund patient care. We are looking for 100 donors to pledge $100 per month for the next year. These funds will help us to cover the costs of our poorest patients. You can set up a recurring gift through our secure site here. God bless you!
Servers and Soddo
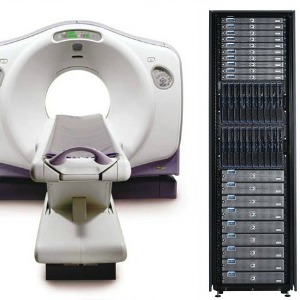
Take a look at these photos:

These are not things that you might be used to seeing in a mission hospital. But the reality is that all hospitals, even mission hospitals, are getting on the technology bandwagon. We have a CT scanner that improves our diagnostics - allowing us to make more accurate diagnoses and provide better care. We have a server room and a network that extends throughout the hospital campus. That allows us to access internet and current treatment recommendations. It gives us the ability to look at digital x-rays and CT images throughout the hospital. And one day, it will allow for an electronic medical record to keep track of our patients.
The mission hospital of the 21st century is not what you thought! We've got a lot of technology, and we've got to keep it all running. If you are a network administrator, computer programmer, IT specialist - or if you know any - come and help us out! We'd love to have you for a short term visit, or longer. Contact us if you're interested.

The Ambulance Is Here!
A few months ago, we posted the project for an ambulance and the need. Well, God answered our prayers, and provided the funds and now, the ambulance!
Just today, the new Landcruiser ambulance was driven down from Addis and on to our hospital grounds by our own chief administrator, Ato Desalegn. Here is Desalegn pictured with Pastor Daniel, the head of our spiritual ministries, by the new ambulance. He even fired up the siren as he pulled on campus to let everyone know.
There's a lot of excitement here around our newest addition. In Ethiopia, there are no municipal-backed EMS systems. So having an ambulance is really key for hospitals. It will allow us to transfer and go pick up sick patients. From time to time, we have had really sick patients who required a specialized operation or procedure only available in Addis Ababa. Before, we had no way to get them there, and some of these patients died. Now, we will be able to take them in our new ambulance.
An ambulance really legitimizes us in the eyes of the people of this area too. People know they will be cared for here, and if for some reason we need to transfer them, now we can!
Thanks to so many of you who helped us reach this goal. We thank God for you!

SCH Graduate Makes History
Recently, the very first graduate from the PAACS program in Ethiopia did something unique in his own country. He led a team that separated conjoined (“Siamese”) twins. To our knowledge, nothing like that had ever been attempted in Ethiopia. Dr. Frehun Ayele, who trained as a pediatric surgeon at the BethanyKids at Kijabe Hospital PAACS program after graduating from the general surgery program in Ethiopia, led a team of surgeons from Myungsung Christian Medical Center to perform the incredibly delicate and complicated operation. The baby sisters were born at a health center in the countryside and were abandoned by their mother. They were given to a Catholic mission group here who then brought them to MCM. One of the twins had a severe, fatal heart defect and it soon became clear that she could not survive. This made transfer abroad impossible because of time considerations, so Frehun made the difficult decision to take them to the operating room to separate them. It was clear that one of the twins would die, sacrificing her life for her sister's. Dr. Frehun concluded that if he did not intervene urgently, both babies would die. The surviving twin, Mariam, is doing well. Please pray for her as she recovers. We praise God for Frehun's faithfulness in serving Him as he serves the sick children of Ethiopia.


Hot Zone in Soddo
Last week, we had some pediatric patients come in with upper respiratory symptoms. A few of them had a rash and had been given antibiotics, so there was a thought that maybe it was a "drug-related rash." But it wasn't long before a few more kids came in, and it was clear that this wasn't a medication-induced rash. Yep, this was measles.


It didn't take long before our entire pediatric ward was full of measles patients. We were in the middle of a genuine outbreak. The feared complication of measles is pneumonia, and indeed most of the patients we were getting had it. Many have them were requiring oxygen. In the picture below, the machines on the floor are oxygen concentrators.

The health department was notified, and they began taking measures. Much of the outbreak was centered on an orphanage down the street from us. So we contacted them and gave them specific instructions. First, isolate any kids that were showing symptoms. Second, send any kids to the hospital that were showing signs of pneumonia or respiratory distress. We took a trip down to the orphanage ourselves to see the patients who were not sent to the hospital and check on them.

By God's grace, the outbreak seems to be relenting. Our hospital has admitted around 15 kids. Sadly, a few of them have succumbed to the disease. The thing about measles in outbreak settings, is that it affects the very young. Children are vaccinated against this virus between nine months and one year of age. So the most vulnerable are the babies less than nine months. Formula-fed babies (like the orphans) are particularly vulnerable because they don't get protective maternal antibodies. Fortunately, some who were very sick are pulling through. The situation itself feels like a war zone. Our doctors and our nurses are tired, but they are doing an amazing job - rising to the occasion and providing excellent care. We praise God for using us in this situation, and hope to bring Him glory through it. As it says in 1 Cor 15:58, "Be steadfast, immovable, always abounding in the work of the Lord, knowing that in the Lord your labor is not in vain." Pray that we will be steadfast. And that no more of these precious little ones will die.
The other thing about situations like this, is that it stretches our thin resources to the maximum. We don't have enough oxygen concentrators. We don't have enough pulse oximeters. And we can't mechanically ventilate kids with severe pneumonia. We hope to buy non-invasive ventilator machines, and perhaps one or two mechanical ventilators. We'd love to be even better prepared the next time this happens. Would you consider a donation today that would help us do that? Just click donate in the upper right corner of the site. Thanks for your support and prayers.

What? You don't have Idraparinux?
What kinds of medications are available at an African mission hospital, and from whom do you procure them? These are questions that we get asked a lot. Here are two lists. Five things we have, and five things we don't! Most of our medications are imported from Europe and Asia. A few are made locally in Ethiopia. One thing we can't use is expired meds - it's prohibited by law - so even though we'd like to take these off your hands, please don't send them to us!
Five medications we have:
- Most antibiotics! We have penicillins, 3rd generation cephalosporins, macrolides, aminoglycosides, fluoroquinolones. We even have vancomycin most of the time.
- Pain meds: For mild pain, we carry ibuprofen and tylenol. We also have stronger IV pain meds for our surgical patients, and fractures.
- Blood pressure and diabetes medications. We have oral calcium channel blockers, ACE inhibitors, diuretics, and some beta-blockers. We use metformin and glibencamide for diabetes control, and we also have insulin.
- Albuterol multi-dose inhalers. These are key for our chronic asthma patients, and COPD patients. We don't have nebulized albuterol (which we'd like to have), but we can substitute these MDIs, and they work quite well.
- GI problems? We've got proton pump inhibitors (Prilosec for example), and we even have Zofran for nausea and vomiting.
Five medications we don't have. We are hoping that in time, our access to some of these meds will improve:
- Fancy antibiotics. Anti-pseudomonal penicillins like Timentin and Zosyn. These are great for severe infections. Also, we still lack a good IV first generation cephalosporin.
- Artesunate. This is the WHO-recommended standard for IV treatment of severe malaria. It is difficult to find however, and we rarely have it. Instead, we use Quinine which is an acceptable but less desirable medication.
- Newer blood pressure and heart failure medications like Carvedilol. Also, newer diabetes meds like long-acting insulins.
- Low-molecular weight heparin. Ever heard of Lovenox? It makes treating deep venous thrombosis and pulmonary embolism so much easier. But alas, it is rarely available on the African market.
- IV calcium and sodium bicarbonate - rarely we will have these. It does create problems managing a hyperkalemic patient or profoundly hypocalcemic patient. We have other therapies that we can use though.
Others you are wondering about? Ask in the comments and we'll respond!